
Prolapse
On this page:
This page provides information about pelvic organ prolapse. If you have any further questions or concerns, please speak to the staff member in charge of your care.
What is a prolapse?
Prolapse is the term used when an organ or structure in the body slips out of its normal position. This can happen when the muscles and tissues that support the organs become weak or stretched. Prolapse can affect different areas of the body, but rectal prolapse and vaginal prolapse are the most common within the pelvic area.
Types of prolapse in the pelvic area
1. Rectal prolapse
This occurs when the rectum protrudes through the anus. This can be partial or full.
Symptoms include bleeding, pain, discomfort and difficulty with completely emptying the bowel.
Partial prolapse – also known as mucosal prolapse is only when the lining of the rectum comes out usually during bowel movements and can be squeezed or pushed back in.
Full thickness prolapse – The entire thickness of the rectal wall protrudes through the anus and will fall out even when squeezed or pushed back in.
Why have I got it?
Rectal prolapse can be caused by several factors. Some of these include:
- Chronic constipation – straining during bowel movements
- Weak pelvic floor Muscles – aging, childbirth, pelvic floor surgery
- Genetic factors – Hereditary conditions like Ehlers-Danlos syndrome, Marfan syndrome.
- Increased pressure – Obesity, chronic coughs, heavy lifting
- Neurological conditions – Spinal cord injury, or MS can affect the nerves which control the bowel.
what can be done about rectal prolapse?
Conservative treatments: Dietary changes (increased fibre), stool softeners, and pelvic floor exercises.
Surgical options: If conservative measures are not effective, surgery may be required to reposition the rectum or strengthen the supporting tissues.
2. Vaginal Prolapse
This occurs when one or more of the pelvic organs (such as the bladder, uterus, or rectum) drop down and push against the walls of the vagina. This is caused by weakening of the pelvic floor muscles and connective tissues that hold the organs in place.
Prolapse is very common and affects around 50% of women who have had a vaginal birth. It can also affect women who have not been pregnant or given birth. Additionally, some cancer treatments can have an impact on the pelvic tissue and pelvic floor muscles which can weaken this area and therefore increase the risk of prolapse.
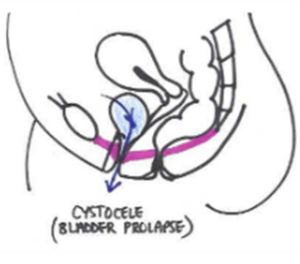 An anterior wall prolapse (previously known as cystocele) is the most common prolapse. It occurs when the bladder pushes into the front wall of the vagina. This may cause difficulty in emptying the bladder which could cause infections. It may also cause an increase in urinary frequency (day or night), incontinence and difficulty in starting the flow of urine.
An anterior wall prolapse (previously known as cystocele) is the most common prolapse. It occurs when the bladder pushes into the front wall of the vagina. This may cause difficulty in emptying the bladder which could cause infections. It may also cause an increase in urinary frequency (day or night), incontinence and difficulty in starting the flow of urine.
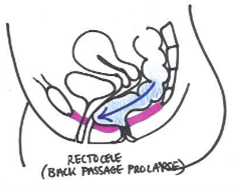 A posterior wall prolapse (previously known as rectocele) occurs when the rectum pushes into the back wall of the vagina. This may cause difficulty emptying or incomplete emptying of the bowels. It may also cause an increase in the sudden urge to empty your bowels or worsen constipation.
A posterior wall prolapse (previously known as rectocele) occurs when the rectum pushes into the back wall of the vagina. This may cause difficulty emptying or incomplete emptying of the bowels. It may also cause an increase in the sudden urge to empty your bowels or worsen constipation.
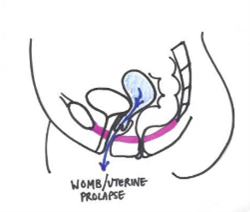 A uterine prolapse occurs when the womb moves down into the vagina due to lack of support. The cervix sits lower in the vagina. This may be noted when you have a smear test, but you may not be aware of the symptoms.
A uterine prolapse occurs when the womb moves down into the vagina due to lack of support. The cervix sits lower in the vagina. This may be noted when you have a smear test, but you may not be aware of the symptoms.
What are the signs and symptoms?
Not all prolapses are symptomatic; however, you might have experienced one or more of the following symptoms:
- Feeling of a bulge or heaviness into your vagina
- Lower back pain
- Urinary or bowel incontinence
- Difficulty emptying bladder or bowel
- Needing to pass urine more frequently
- Pain or discomfort during intercourse
Why have I got it?
Prolapse can be caused by several factors which affect the support system of the vagina. Some of the main factors that can contribute are:
- Pregnancy and childbirth
- Surgery impacting the muscles and nerves of the pelvis
- Treatments which lead to oestrogen deficiency
- Pelvic floor muscle weakness
- Obesity and being overweight
- Constipation – chronic straining
- Heavy lifting
- Family history
- Age
- Menopause and hormonal changes
- Chronic respiratory conditions
- Previous pelvic surgeries
What can I do about it?
Pelvic organ prolapse is not life threatening and with the correct management may improve. These are some of the options for management of your prolapse:
- Adopt good bladder and bowel habits and try to avoid constipation. For more information, visit our pelvic health page.
- Reduce heavy lifting where possible.
- Avoid long periods of standing or take short breaks if you are unable to avoid this.
- Maintain a healthy weight – we know that being overweight increases prolapse symptoms for multiple reasons. There are many resources on the NHS website for weight management. If you are struggling with this speak to your GP for further help.
- Improve your pelvic floor muscle function by completing pelvic floor exercises that focus on strengthening and relaxing your muscles
- Your GP may discuss other options with you such as a vaginal support pessary or oestrogen treatment, or refer you to a gynaecologist for further management
It may take between 6-12 weeks of consistent pelvic floor strengthening before you notice any improvement in your symptoms. This might seem like a long time; however, it is important you persevere as these exercises can make a significant difference to your symptoms.
Can I still exercise?
Yes. Exercise is important and appropriate exercise can improve your symptoms. Some activities are known to cause an increased pressure on your support systems including your pelvic floor.
If you are experiencing prolapse symptoms during a certain activity, it is advisable to modify this activity until your pelvic floor is strong enough to withstand the increased pressure. You should only continue with this activity once it no longer worsens your prolapse symptoms. These activities commonly increase the pressures:
- High impact exercise – for example jumping, running, HIIT. You could consider temporarily replacing these with swimming, cycling, Pilates, yoga, fast walking, or other low impact exercise.
- Heavy lifting – this could include carrying your food shopping home, lifting and carrying toddlers, long walks with a baby carrier on, or lifting weights in the gym.
- Think about reducing loads and modifying daily activities whilst you are improving pelvic floor strength. Sometimes lifting is unavoidable, in these instances try squeezing and holding your pelvic floor muscles through the lifting action.
- Finally, during any exercise it is important that you do not hold your breath. Try breathing out on exertion.