Acute Kidney Injury (AKI) Clinic
On this page:
The Acute Kidney Injury (AKI) Clinic is a specialist Nephrology-led service, which opened in 2012. The service aims to improve prevention, early detection and management of AKI by providing advice and education to the multidisciplinary team. We support identification and monitoring of patients with AKI – from diagnosis to discharge – and provide an outpatient follow-up service.
The AKI clinic runs twice-weekly on Tuesdays afternoons in Richmond Ambulatory Assessment Area to focus on AKI admission avoidance, and on Friday mornings in Lanesborough Clinic A for follow-up patients with AKI.
 What we do
What we do
In clinic, the AKI team:
- explains what AKI is and the likely cause for the AKI episode
- undertakes a physical assessment, including blood pressure, urine dipstick and examining for signs of fluid overload
- reviews the patient’s renal autoimmune disease and myeloma screens, where appropriate, to ensure nothing has been missed which requires follow-up
- reviews the patient’s medications to assess whether medications stopped due to the AKI can be reinstated
- will assess whether the patients’ kidney function has returned to normal. This will normally require a specific blood test around the time of the appointment
- will arrange further imaging or investigations, as required
- will advise about prevention/progression of chronic kidney disease (CKD), including healthy lifestyle choices, smoking cessation and the avoidance of nephrotoxins, especially NSAIDs.
- will provide a simple information leaflet which includes all of this advice
After reviewing the patient’s bloods following the clinic appointment, if the creatinine remains elevated or an abnormal renal disease screen is identified, the patient is referred on to the General Nephrology clinic. Otherwise patients are discharged back to GP care with advice on monitoring in line with the NICE CKD guidelines.
When to refer
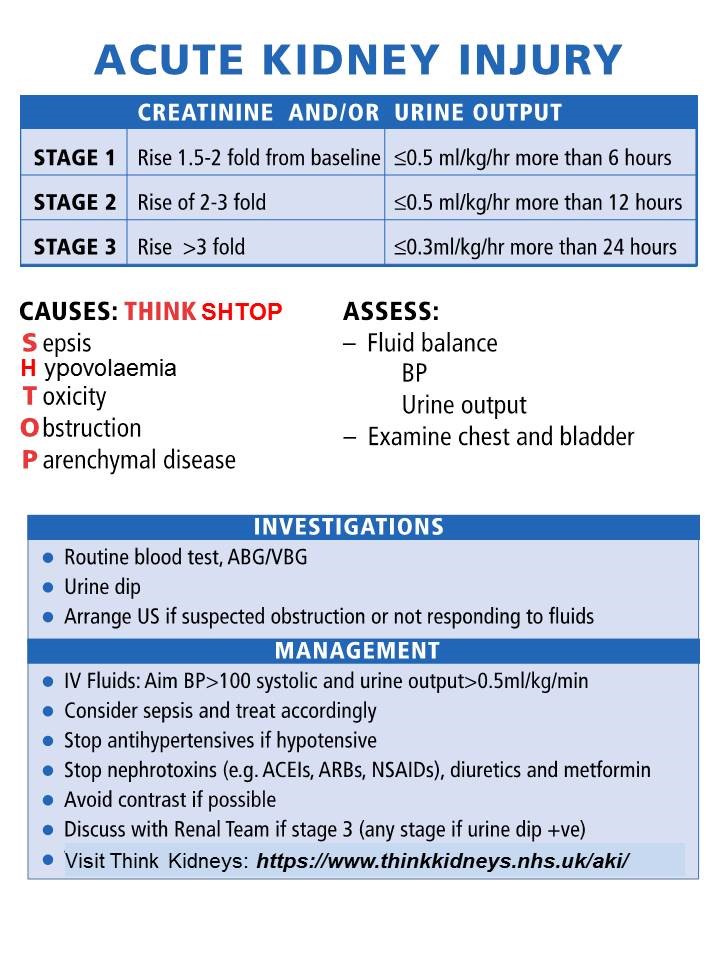
See think kidneys guidance for identification and first steps management guidelines available here.
Referral criteria from Primary and Secondary Care include:
- New AKI stage 1 or 2 in clinically stable patients
- Recovering AKI in patients with AKI stage 1, 2 or 3 (excluding kidney transplant patients)
- Reintroduction of prognostically beneficial medications (including ACE inhibitors/ARBs) following an AKI episode.
Timeframe for response to e-Alert
| AKI | Stable | Acutely unwell |
| Stage 1 | < 72 hrs (telephone review) | < 24 hrs |
| Stage 2 | < 24 hrs | < 6 hrs |
| Stage 3 | See < 6 hrs, Admit | Admit |
How to refer
To discuss a patient:
AMU Consultant Bleep 7915 (Mon-Fri 9am-9pm)
Renal SpR Bleep 6415 (Mon-Fri 9am-5pm; out of hours/weekends via St George’s Hospital Switchboard 020-8672-1255)
Email: akiclinic@stgeorges.nhs.uk (all referrals)
AKI Clinical Nurse Specialist: Bleep 6005; Ext 0360 (Mon-Fri 8am-4pm)
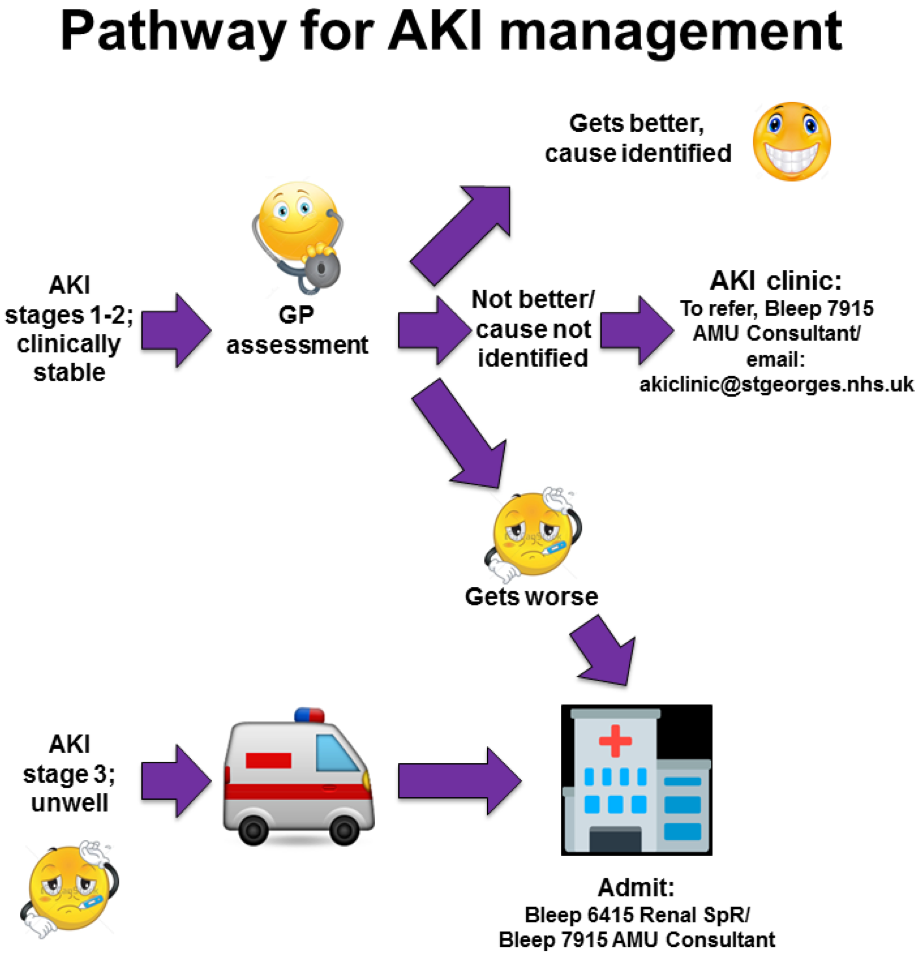
Pathway for AKI Management